
Thyroid Problems

Dr David Richardson
Thyroid problems are very common especially in women. Probably at least 20% of women over 60 have some degree of underactive thyroid. Minor degrees of hypothyroidism are often undiagnosed. TSH is reported as normal in Australia if it is less than 4.5. Yet people with TSH > 2.5 may have subclinical hypothyroidism.
Subclinical Hypothyroidism
Most Australian endocrinologists feel this subclinical hypothyroidism has minimal effect on their patients. However, these patients are often over 50, and already have declining sex hormone levels and increasing age related change. Adding suboptimal thyroid function to this mix may certainly contribute to feeling “old before their time”, or that they are not as well and vital as they were a decade earlier.
Most thyroid decline is probably autoimmune in cause, but for people with symptoms consistent with underactive thyroid and raised TSH it is always worth checking iodine levels with a urine test.
Then iodine can be supplemented, and some herbal mixes e.g. Metagenics Thyrotone or similar may help. There are subtle links between declining sex hormones and lower thyroid levels too, and attending to sex hormones with BHRT often seems to boost thyroid function.
Occasionally prescription thyroid replacement is necessary for subclinical hypothyroidism.
Autoimmune hypothyroidism
This is the commonest cause of full hypothyroidism in Australia, then surgical removal of part or all of the gland.
These types of underactive thyroid are usually successfully treated with the thyroid hormone T4 (Thyroxine), and this works well probably in 80-90% of people with these problems. Ideally TSH is about 0.5-1.5, and if you are on thyroxine and you are listless or have other symptoms of underactive thyroid it is reasonable to ask your doctor to try to keep your TSH in this ideal range. Why not get things back to optimum!
However there do seem to be a small group of people who still feel as though their levels are too low even when their TSH is very suppressed, say < 0.1.
These people are unfortunately often not served well by their GPs or endocrinologists who may deny their symptoms or imply they are imagining them.
I believe these people are often actually overdosed on T4 by their well meaning doctors.
Reverse T3
T4 is converted by the liver to T3 (triodothyronine) which is the active version of the thyroid hormone. Some people make large amounts of RT3 (Reverse triodothyronine).
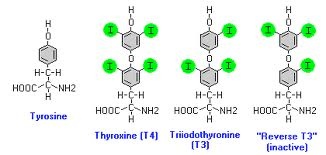
My goal is to achieve RT3 levels of 350 or less.
We can do this by giving a little T3, and reducing T4, which results in less T4 being converted to RT3, and higher T3/RT3 ratios.
This balancing act makes thyroid replacement therapy more complex, but for the small group of patients not served well by conventional thyroid replacement it often seems to make a world of difference.